


Wake Me Up When September Ends II: perspective is only useful when used
The coming winter wave & default conclusions

Note: **My new Prometheus Hub page** compiles most of the research and resources I’ve used/found/analyzed/watched/etc. during [and prior to] my efforts with DRASTIC, so that those who are looking for more about COVID’s origins can find it in one place.
I don’t plan on ever charging a subscription fee for any of the content on my site; everything I keep here is the result of 18 months of research conducted because it needed to be done and very few were doing it. However, this has literally been my full-time job since March 2020, so any ‘subscription’ as a donation will help me continue this work uninterrupted by the real world.
Or, if you’re still in the recovery phase of the financial pandemic, spreading the word could be just as helpful to the cause; after all, everyone has suffered from the lack of honest & unbiased information from our leaders that would’ve helped us be clear-eyed about what we were going to face. I have no greater responsibility with this site than to keep it accessible to anyone who deserves the truth - which, of course, is all of us.
or
This will be followed shortly by another article that serves as an analysis of this and the data regarding vaccine efficacy and usage. But, it’s important to understand where we came from to understand where we’re going.
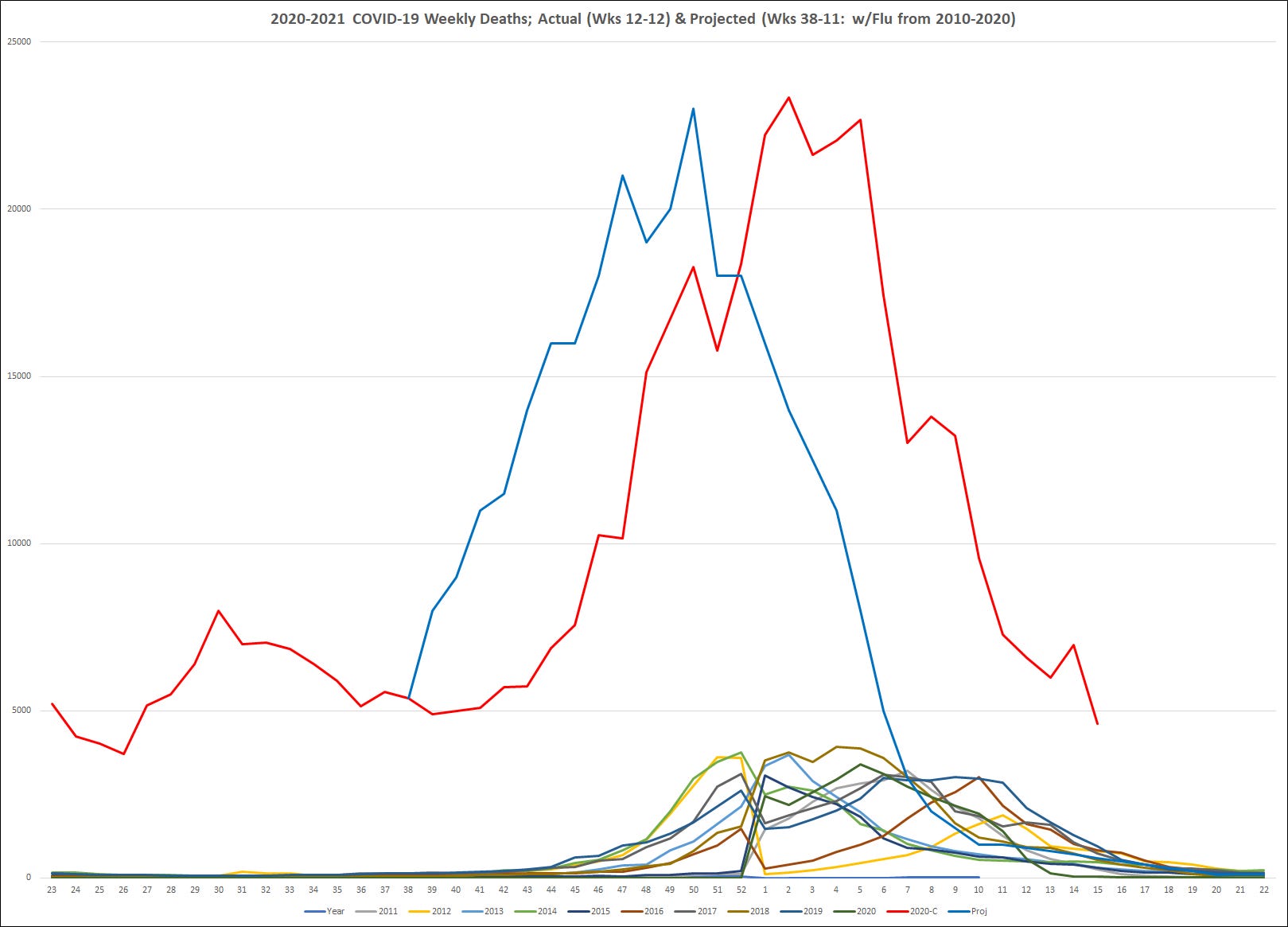
I published this article on October 7th, 2020, after being frustrated that our US federal government had basically abdicated any desire and responsibility to provide a realistic assessment of what was going to happen in the fall of 2020. It should be noted that in addition to being roughly 2,000 deaths off from the true value on May 1st [prior to the rise of the delta variant], my projection did not include any variables like lockdowns, mask usage, etc. I’d say that speaks volumes about their relative importance in effecting overall outcomes in the pandemic.
Perspective, Projections and Protection for COVID-19: Analyzing what we've seen, where we are going, and emerging insights that can help us reduce the impact of the 2nd Wave.
As the potential Big Wave approaches, our hindsight is clearing up - but that only helps if we use it.
[Calculated 9/27/20; Published 10/7/20]
I: "A Strong Flu"
-5 months ago, I published the article "Wake Me Up When September Ends;" although the title was a reference to a 2005 song by the band Green Day, the content was an analysis of the CDC's five decades of statistics that tracked the impact of annual influenza outbreaks. The first two articles I wrote for my COVID-19 info site had focused on estimating the disease's infection fatality ratio (IFR), because an accurate value for any virus's lethality increases the accuracy and effectiveness of the public health measures implemented as a response (see The Corona Conundrum I and II). What stood out to me most were the frequent characterizations of COVID-19 as 'a strong flu.' The image above shows the weekly death totals of COVID-19 compared with the same statistic from the last 10 flu seasons, and I feel like the image speaks for itself.

-The politically inclined reader may have already guessed the reason why the CFR/IFR is a sexy statistic - it is highly correlated with the overall size (and cost) of a central government's response, while also having a powerful influence on projections of future infection spread. Here in the US, the inaccuracy of early projections from the University of Washington (used by the White House) and many other official sources likely accelerated the polarization of the pandemic response, by telegraphing scientists' uncertainty and opening the door for 'interpretations' of the statistics.
-I have spent the last 7 months trying to weed through those interpretations to better understand what the pandemic actually looks like, because it's been very easy to miss the big picture when numbers blur together without context. For example, everyone knows the US has led the world in cases and deaths, but practically no one is aware that our CFR is actually below the global mean; the only time it exceeded that number was in April. In Portraits of a Pandemic, I pointed out the impact of that statistic:

-It's worth pointing out that it wasn't the smaller countries struggling, it was the big ones: the UK, France, Italy, Germany, Spain, Denmark, etc. Critics here and in Europe have been brutal in assessing the administration's handling of the crisis, but the US stands far closer to herd immunity at 1/3 the human cost, by proportion.
-As a final note before offering my projection of what Fall could look like, the pie chart below represents the most disturbing anomaly I found when combining 44 years of CDC flu data to analyze trends in the impact of winter on infection rates and mortality. The 'novel' character of SARS-CoV-2 has rightfully led to comparisons with H1N1, the last such pandemic threat. And, since the early summer, the broad scientific consensus has considered COVID-19 to be 'seasonal' just like the majority of respiratory virus-infections, and the focus turned to planning for that surge.

If the consensus is proven correct, then this chart should dispel any last notions of COVID-19 as a "Strong Flu." The average off-season from June-September produced 3.04% of deaths when added to the total for the June-May flu 'year.' On an average summer day from 1976-2019 (when the CDC records begin), 7 people died from the flu; in 2020, COVID-19's daily average was 824. After taking the 12.34% increase in average deaths/decade backwards, 16 weeks of COVID-19 killed more people than every summer since 1919 - 101 summers of 16 weeks each. The SARS-CoV-2 virus produced more than a century's worth of deaths during the slowest time of the year, despite an unprecedented lockdown. Perhaps the most disturbing realization for me is the fact that I found the data while looking for something else; an extra hour of my time is the only reason you see it now. I wonder what the chart might've looked like had any media framed the pandemic like this two months ago?
II: Projecting Hurricane Pandora-19's Path
-This time, I'll lead with the chart of my (rough) projection (updated as of 12/12):

As of this minute on 10/7, the US confirmed death count is 210,874. Ultimately, this chart depicts a curve leading to 500,542 confirmed deaths by May 31st - a figure stemming from the same basic trends as my 200K prediction for 10/1 that I made in May:

{Reflections of a more personal nature have been omitted; the later comparison with Swine Flu was calculated as if infections were spread in exact proportion to the age distribution of the US, an example scenario that would have an age-adjusted 1.9% IFR}
I had no desire for my prediction to come true; I simply wanted to provide an unbiased assessment since it seemed obvious that our media wasn't very interested in providing one. I wanted to leverage any small amount of past experience I could to tell others the same thing I had told my family in March - that regardless of whatever background noise they might hear, the COVID-19 story was not going to end any time soon.
-My starting assumption was that the general course of COVID-19 will keep holding to a pattern resembling the spread of H1N1, rather than typical seasonal flu, even though it is more deadly and more contagious. One primary reason is that social distancing and cloth masks do have an impact, even if the pace of COVID-19 infection has matched or exceeded that of the Swine Flu. Under-estimating the problem (infectivity rates) would naturally make a solution appear less effective. Another reason would be the fact that both 'novel' pandemics were detected in late December/early January and continued to progress throughout the year. The CDC estimated that H1N1 infections stood at 22 million in early October and doubled to 44 million in the next 6-8 weeks; the salient detail (from my perspective) is that H1N1 peaked earlier than normal flu strains, thanks to a six-month head start during the previous season.
-COVID-19 entered October with an unknown number of US cases, but my current IFR estimate (based on methods discussed in my linked articles above) is roughly .84%, which happens to work out to an estimated true infection number of 32.7 million Americans [10.0%] as of today:

There's more to process in this image than I can fit into a LinkedIn article, but my estimates are based on confirmed deaths, which has always been the best statistic to start with since it's the only variable with enough evidence for us to determine a value with any accuracy. I should clarify that 'us' in this context refers to the Centers for Disease Control (CDC), not my personal opinion; the CDC has been tracking the "excess deaths" as well as the base COVID-19 statistics, which is the reason that my 500,422 projection for confirmed deaths is less than my overall 616,366 estimate. I simply added the 50% of the CDC's current excess death estimates and assumed that the 23.17% proportion of excess deaths to the total COVID-19 count would remain static (50% is actually lower than what the CDC attributes to the virus).
-Among my other assumptions, I expect that the CFR will not drastically rise above current levels, because during the wave that hit the 3 most populous states simultaneously in late June, mortality rates continued to fall instead of spiking like New England's did. I actually raised my upper-range estimate for October to 300K+, because I assumed that New York's 8% CFR was mostly driven by a lack of hospital capacity - but California, Texas and Florida mortality rates were 1/3 of New York's despite a higher proportion of their populations becoming infected. If this is simply a product of weather, then the winter will lead to a narrower CFR gap; my projection assumes that the real difference is a mixture of temperature, better understanding of the virus and mismanagement in the pandemic's early stages.
-With these and other considerations, my long-term outlook implies that COVID-19 will peak before 2021, and that we will see a doubling of cases and deaths similar to H1N1 - though the process should take longer given social distancing measures. COVID-19's greater lag time between infection and death could push the peak back a few weeks, but for now my guess is that it will come in early December. Infections should fall in January 2021 as the gravitational pull of vaccines and a diminishing proportion of unexposed people lead to a lower reproduction rate. In December 2009, I experienced this firsthand, after flying home for Christmas only for my wife and 3 kids to all contract H1N1 in that two-week span. I find it very likely that I avoided their fate because, as an active duty Marine, my flu vaccine cocktail included the new H1N1 strain. If distribution of COVID vaccines begins around the start of the new year, deaths should correspondingly decline 2-3 weeks later, falling at a faster rate because of the reproduction rate pressure.
III: Fighting Back: The Good News You Haven't Heard
-This forecast could significantly shift if the SARS-CoV-2 virus mutates like the Spanish Flu in 1918, no vaccine is ready for approval by January, or multiple portions of the country experience a New York-style overload during the peak. However, the mutation rate of the virus is far lower than expected - one of the primary questions that makes determining COVID-19's origins so important. Several vaccines remain on course to complete phase 3 trials soon, per the NYT's tracker, and last week President Trump was treated with monoclonal antibodies, the same therapy I highlighted in this article's namesake on May 11th.
-Deciding to offer a long-term projection was not an easy decision for me, because I saw how much the public was affected by the obvious uncertainty of our experts' early prognoses. 7 months later, however, the situation has changed. The longer the pandemic stretches on, the more important preparation and realism become; Americans need to hear the range of possible outcomes so that acceptance can turn into determination. There are many reasons for politicians of all stripes to avoid clarifying what is likely to happen next, especially with an election a month away - setting any expectations would be sobering for voters, and avoiding them keeps criticism from scrutiny. It's vey easy to make every response look like a failure when there's no context, but context is exactly what citizens need to gain a clear perspective. I intentionally avoided other projections after deciding to write this piece, and before then other aspects of the pandemic were my focus. I wanted to base my picture on the data and research, not on something which would paint a picture that supported a desired point-of-view. If the numbers on January 1st are 300,000 instead of 400,000 , I will rejoice in my mistakes.
But at it stands, Americans have no context from which to know whether to celebrate or mourn that outcome - and the last 7 months have made it clear that without context, our leaders are condemning us to further anguish, because without evidence, the default conclusion is to mourn.
C.H. Rixey, 10/7
9/4/21 update:
The US passed 200,000 confirmed deaths on 9/23/20; 300,000 on 12/11; 400,000 on 1/17/21; 500,000 on 2/22 and 600,000 on 6/17.
It’s important to point out that this doesn’t include excess deaths, which is why the 600K threshold wasn’t crossed until June. I’ll discuss this in depth in the next article in this series - and I’ll also discuss my latest findings regarding vaccines - a rising case fatality rate among the most highly-vaccinated states. The implications of that dichotomy have not been publicly discussed, and that is disturbing. I originally just wanted to highlight how much our federal government failed to use its resources to warn Americans about what last fall was going to look like. However, our current course has the possibility of magnifying the mistakes we should’ve already learned from.
R/S,
Charles
I’ll leave you with a snippet of the results from my projection. I’m hoping that my larger platform can put more attention on the topic I’m currently writing about than this did a year ago. Once again, I hope I’m wrong.
